What is cataract & how it forms?
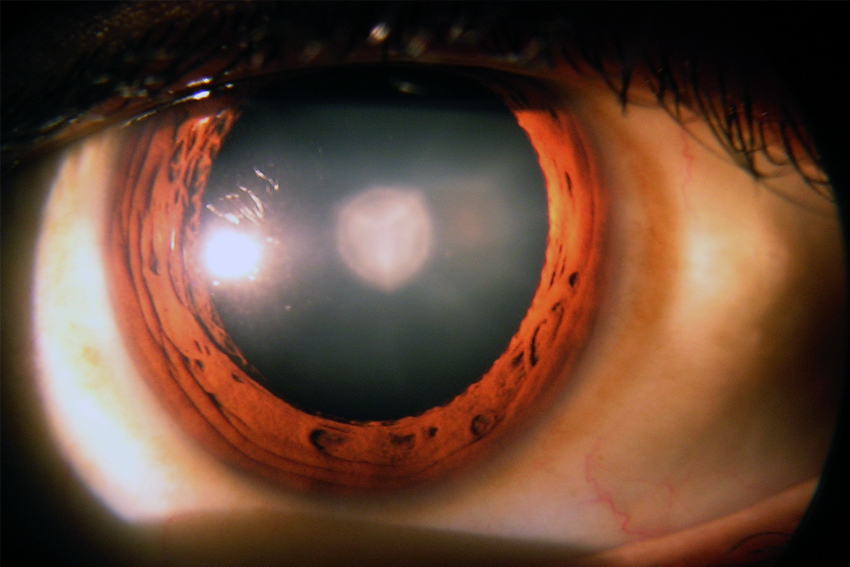
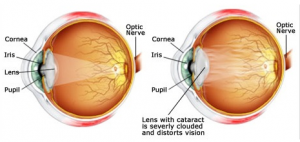 The lens, where cataracts form, is positioned behind the colored part of your eye (iris). The lens focuses light that passes into your eye, producing clear, sharp images on the retina — the light-sensitive membrane on the back inside wall of your eyeball that functions like the film of a camera. A cataract scatters the light as it passes through the lens, preventing a sharply defined image from reaching your retina. As a result, your vision becomes blurred. As you age, the lenses in your eyes become less flexible, less transparent and thicker. Age-related changes cause tissues within the lens to break down and clump together, clouding small areas within the lens. As the cataract continues to develop, the clouding becomes denser and involves a greater part of the lens. Cataracts may develop in only one eye, but they usually develop in both of your eyes. However, the cataracts usually aren’t totally symmetrical, and the cataract in one eye may be more advanced than the other.
The lens, where cataracts form, is positioned behind the colored part of your eye (iris). The lens focuses light that passes into your eye, producing clear, sharp images on the retina — the light-sensitive membrane on the back inside wall of your eyeball that functions like the film of a camera. A cataract scatters the light as it passes through the lens, preventing a sharply defined image from reaching your retina. As a result, your vision becomes blurred. As you age, the lenses in your eyes become less flexible, less transparent and thicker. Age-related changes cause tissues within the lens to break down and clump together, clouding small areas within the lens. As the cataract continues to develop, the clouding becomes denser and involves a greater part of the lens. Cataracts may develop in only one eye, but they usually develop in both of your eyes. However, the cataracts usually aren’t totally symmetrical, and the cataract in one eye may be more advanced than the other.
Extracapsular cataract extraction involves the removal of almost the entire natural lens while the elastic lens capsule (posterior capsule) is left intact to allow implantation of an intraocular lens. It involves manual expression of the lens through a large (usually 10–12 mm) incision made in the cornea or sclera. It is very rarely done now a days only indicated for patients with very hard cataracts or other situations in which phacoemulsification is considered to have potential problems
Disadvantages
- Long recovery period 4- 6 weeks
- Stitches are required
- Need injection anasthesia
- Higher risk of intraoperative complications
- Higher incidence of postoperative astigmatism with increased dependence on glasses
- Higher chance of posterior capsular opacification and need for laser capsulotomy
This technique is an evolution of ECCE (see below) where the entire lens is expressed out of the eye through a self-sealing scleral tunnel wound (5-6 mm) . An appropriately constructed scleral tunnel is watertight and does not require suturing. The "small" in the title refers to the wound being relatively smaller than an ECCE, although it is still markedly larger than a phaco wound. The advantage of this technique is low cost.
Disadvantages
- Recovery period is about 3 weeks
- Need injection anesthesia
- Higher postoperative surgical induced astigmatism compare to phacoemulsification
Femtolaser cataract surgery is an advanced, blade-free technique that uses a precise laser to perform key steps of cataract removal with exceptional accuracy. It enhances safety, consistency, and visual outcomes compared to traditional methods, offering a smoother and more customized surgical experience.
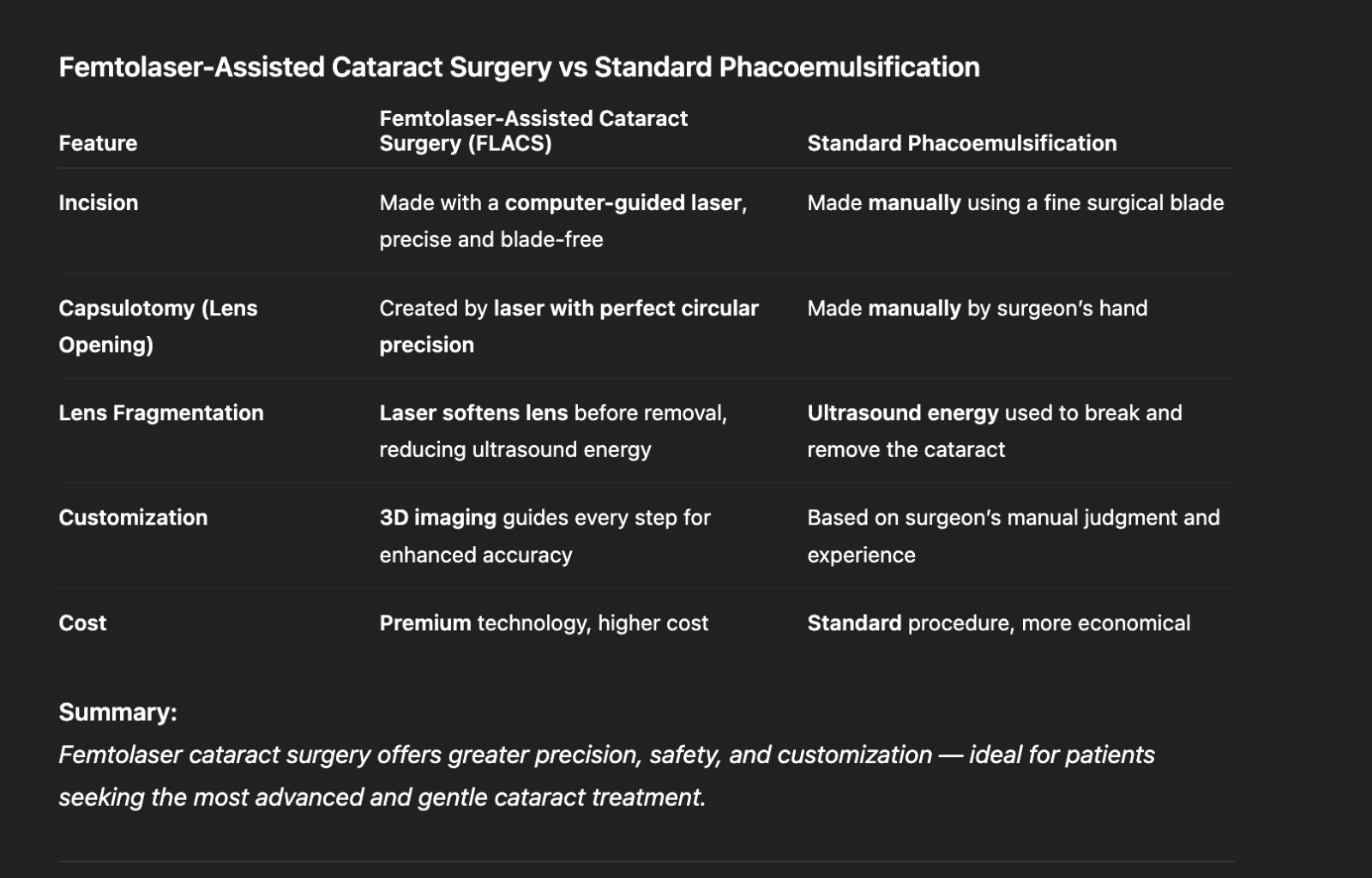
A keyhole incision only 2.2- 2.8 mm wide is made on the outside of the eye. A circular opening in the lens capsule exposes the cataract. Next the phaco-emulsifier is inserted. This sophisticated instrument uses high-speed ultrasound waves to break the cataract into tiny pieces which are suctioned out of the eye.
Advantages
- Recovery time is 2 weeks leading to faster visual rehabilitation
- No injection required – done under topical anesthesia
- Minimal postoperative surgical induced astigmatism

The central and peripheral portion are of the same material.

Then central and peripheral portion are of different material . Advantage of this lens is that it can be used in patient who develops a complication like posterior capsular rent.


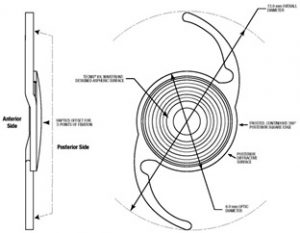
Traditional IOLs are spherical which means the front surface of the the lens is uniformly curved. Aspheric IOLs are slightly flatter in the periphery and designed to provide better contrast sensitivity such as the whereas aspheric intraocular lenses are slightly flatter at the edges to provide better contrast sensitivity. This allows images in a similar color to their background to be more clearly defined.


Toric IOLs are best for patients with significant astigmatism who desire less dependency on glasses.Because they also correct patients' astigmatism, toric IOLs will allow improved distance vision without glasses.
The weakness that toric IOLs share with standard monofocal IOLs is that they are monofocal, allowing either distance vision or reading vision, but not both distance and reading without glasses (unless monovision is employed). Toric IOLs work best with symmetric astigmatism, but they do not correct irregular astigmatism from corneal scarring or other corneal abnormalities. One possible weakness of toric IOLs is that the orientation of the IOL within the eye is critical to addressing the astigmatism. If the lens is not oriented in-line with the astigmatism, the toric IOL may not correct as much astigmatism as it should, and it may even add to the preexisting astigmatism.
EDOF lenses are advanced intraocular lenses that provide clear vision across a wider range — from far to intermediate — reducing dependence on glasses after cataract surgery. They offer smooth, natural vision for daily activities like driving, computer use, and watching TV, with fewer halos and glare than traditional multifocal lenses.

Trifocal lenses are premium intraocular lenses designed to give clear vision at all three distances — near, intermediate, and far — minimizing the need for glasses after cataract surgery. They help patients read, use digital devices, and see distant objects with equal clarity, offering a truly spectacle-free lifestyle for most daily activities.

These are the latest generation of IOL where patients with more than 0.75 diopter preexisting astigmatism can be treated with these lenses to get good unaided distance and near vision
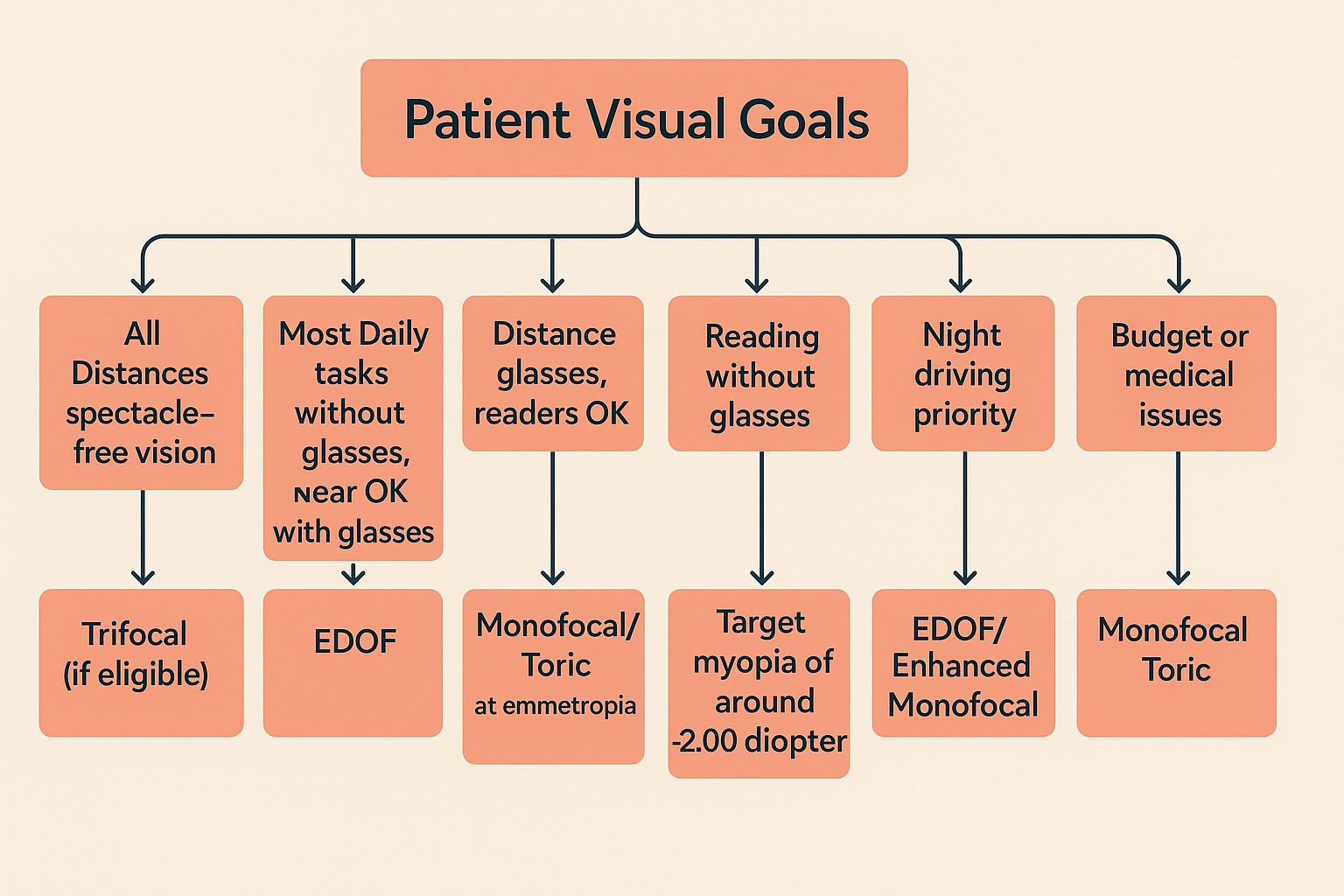
IOL Decision Making
Choosing an IOL is a difficult decision for any patient. The following flow chart is a simplified way of approaching about the question of which lens to implant.